
Chapter 3 – Respiratory System
Posterior and Lateral Thorax – Percussion
The steps in percussing the posterior and lateral thorax are as follows (see Video 3.8):
1. Ensure the client is in an upright position, and perform indirect percussion to evaluate the elicited sounds.
- The lung is an air-filled organ, so the normal percussion note over the lungs of older children, adolescents, and adults is resonance, which is a low-pitched and hollow sound. With very young children under the age of about 5, you will hear a lower-pitch and booming sound (this is described as hyperresonance).
- Listen for any abnormal percussion notes such as dull notes that can occur when the lung tissue is filled with fluid or solid matter (e.g., a tumour close to the chest wall, pneumonia, pleural effusion, atelectasis) or hyperresonance with lung conditions that lead to hyperinflation of part or all of a lung (e.g., emphysema, pneumothorax). Percussion does not elicit reliable data when a client is overweight or obese because the adipose tissue modifies the normal resonance to a dull note. However, the notes typically don’t change with a client who is underweight. Keep in mind that you should not percuss over ribs or the heart. If you do, the sound elicited over the heart (a dense organ) will be a dull high-pitched sound that quickly stops and over the ribs (composed of bone and cartilage will be a flat high-pitched sound that stops promptly with a very short duration). If abnormal percussion sounds are noted, describe the sound and identify the location. Then, perform a complete focused assessment on the respiratory system and check for other related cues.
2. Percuss in about four to eight locations on each side of the posterior thorax and then at three locations on the right lateral thorax and at two locations on the left lateral thorax. See Figure 3.14 for the percussion pattern. Remember that the number of locations depends on the size of the thorax; less locations are needed on a client with a smaller thorax (e.g., infants). Also remember that the posterior thorax is primarily lower lobes.
3. On the posterior thorax, begin at the shoulders at the scapular line. As you move down the thorax, place your finger close to the vertebral line to avoid percussing over the bone of the scapula. Toward the bottom, percuss close to the vertebral line and then move laterally.
- Avoid percussing over ribs because this will elicit a flat note and does not provide you with any important information. You can rock your finger back and forth to ensure you are in an intercostal space. Typically, you will skip the percussion step when the client has a muscular chest or a lot of adipose tissue as this will modify the normal resonant sound to a flat sound. However, a client who is underweight will typically still have a resonant sound.
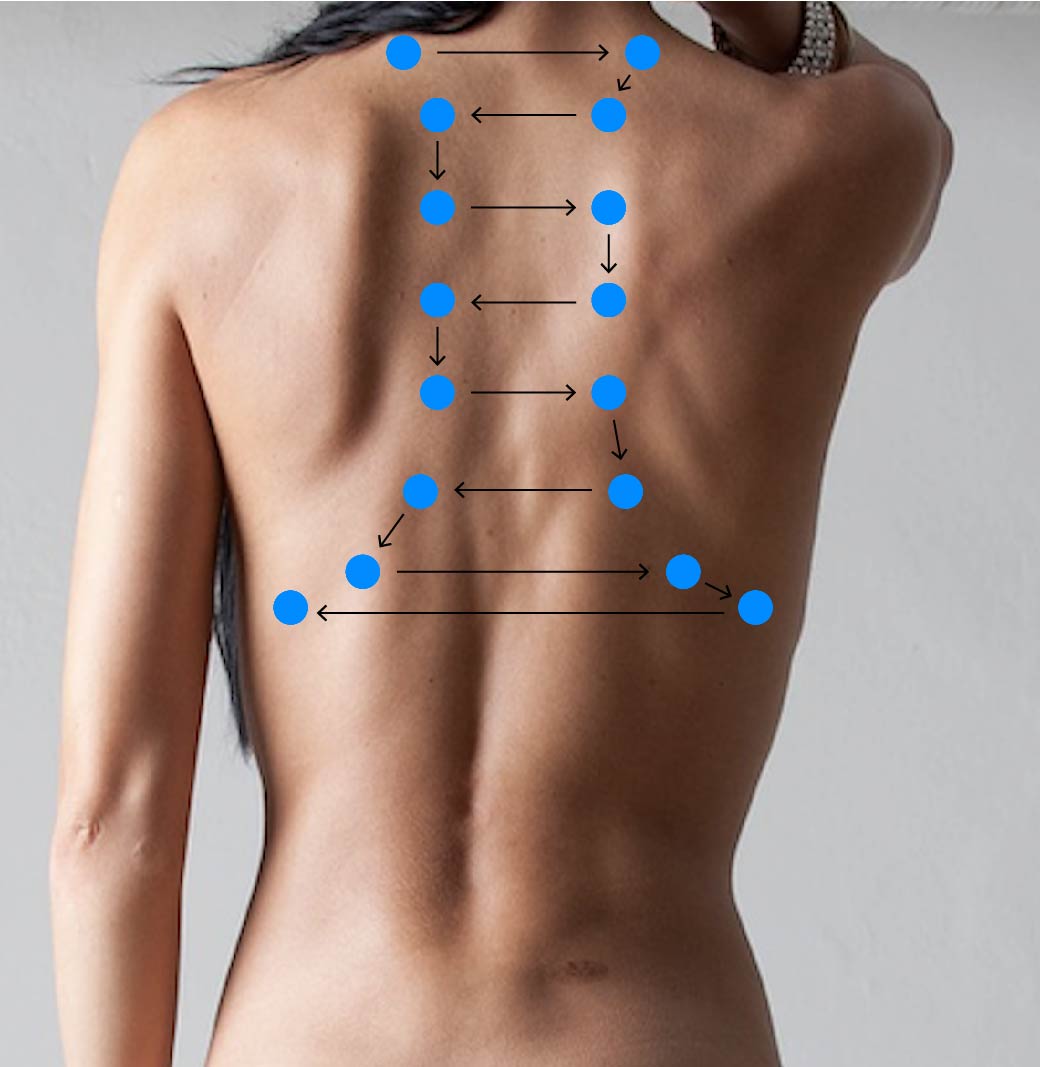
Figure 3.14: Percussion pattern for posterior thorax
Image by Claudio_Scott from Pixabay (image was cropped and illustrated upon for the purposes of this chapter)
4. On the lateral thorax, begin percussing inferior to the axilla and percuss in about three locations on the right side and then two locations on the left side (see Figure 3.15).


Figure 3.15: Percussion pattern for lateral thorax
5. Note the findings
- Normal findings might be documented as: “Resonance heard through lungs on posterior and lateral thorax.”
- Abnormal findings might be documented as: “Resonance heard throughout except hyperresonance heard in left lower lobe on posterior and lateral thorax.”
Video 3.8: Percussion of posterior and lateral thorax (NOTE: percuss down to just below the bottom of the thorax)
Activity: Check Your Understanding
